Over-Diagnosis And Over-Treatment Of Cancer In America Reaches Crisis Levels
Debate Among Doctors Looks at Whether Zealous Screening Leads to Over-treatment. Over-Diagnosis And Over-Treatment Of Cancer In America Reaches Crisis Levels
Early detection has long been seen as a powerful weapon in the battle against cancer. But some experts now see it as double-edged sword.
Related:
Ultimate Guide To Financial Resources For Cancer PatientsFighting Cancer By Releasing The Brakes On The Immune System
Commercial Launch Of Liquid Biopsy Test For Lung Cancer
He Conquered Cancer, Then 15 Spartan Races In A Year
Parabens: A Cancer-Causing And DNA-Damaging Preservative Used In The Food And Cosmetic Industries
Billionaire is Turning Heads With Novel Approach To Fighting Cancer
While it’s clear that early-stage cancers are more treatable than late-stage ones, some leading cancer experts say that zealous screening and advanced diagnostic tools are finding ever-smaller abnormalities in prostate, breast, thyroid and other tissues.
Many are being labeled cancer or precancer and treated aggressively, even though they may never have caused harm.

As a result, these experts say, many people may be undergoing surgery, radiation, chemotherapy and other treatments unnecessarily, sometimes with lifelong side effects.
Meanwhile, an estimated 586,000 Americans will die of cancer this year—many from very aggressive, fast-moving cancers that develop between screenings and spread too quickly to stop.
“We’re not finding enough of the really lethal cancers, and we’re finding too many of the slow-moving ones that probably don’t need to be found,” says Laura Esserman, a breast-cancer surgeon at the University of California, San Francisco.
Dr. Esserman chairs a National Cancer Institute advisory panel that is calling for major changes in how cancer is detected, treated and even talked about. Among its suggestions: devise new screening programs to target the deadliest cancers; create registries to track lower-risk cancers; and remove the term cancer from very slow-growing and precancerous tumors that are unlikely to progress.
The panel suggests calling them “indolent lesions of epithelial origin,” or IDLEs, instead.
“Unfortunately, when patients hear the word cancer, most assume they have a disease that will progress, metastasize and cause death,” the group wrote in the journal Lancet Oncology in May. “Many physicians think so as well, and act or advise their patients accordingly.”
The new thinking could bring radical changes to the vast world of cancer care, which accounts for more than $100 billion in medical costs in the U.S. annually. It is being embraced by a growing number of medical associations and major journals.
“The harm of overdiagnosis to individuals and the cost to health systems is becoming ever clearer,” says Fiona Godlee, editor in chief of The BMJ, formerly the British Medical Journal, which is hosting a conference on the topic starting Monday at Oxford University.
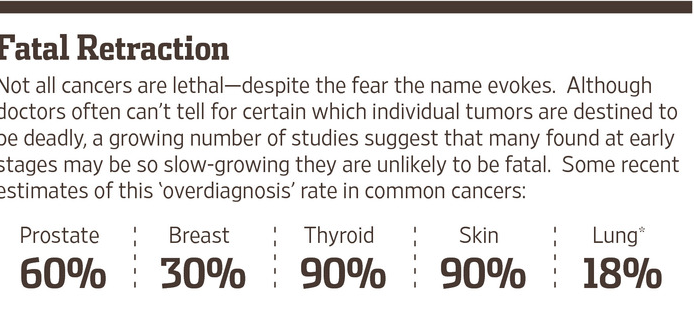
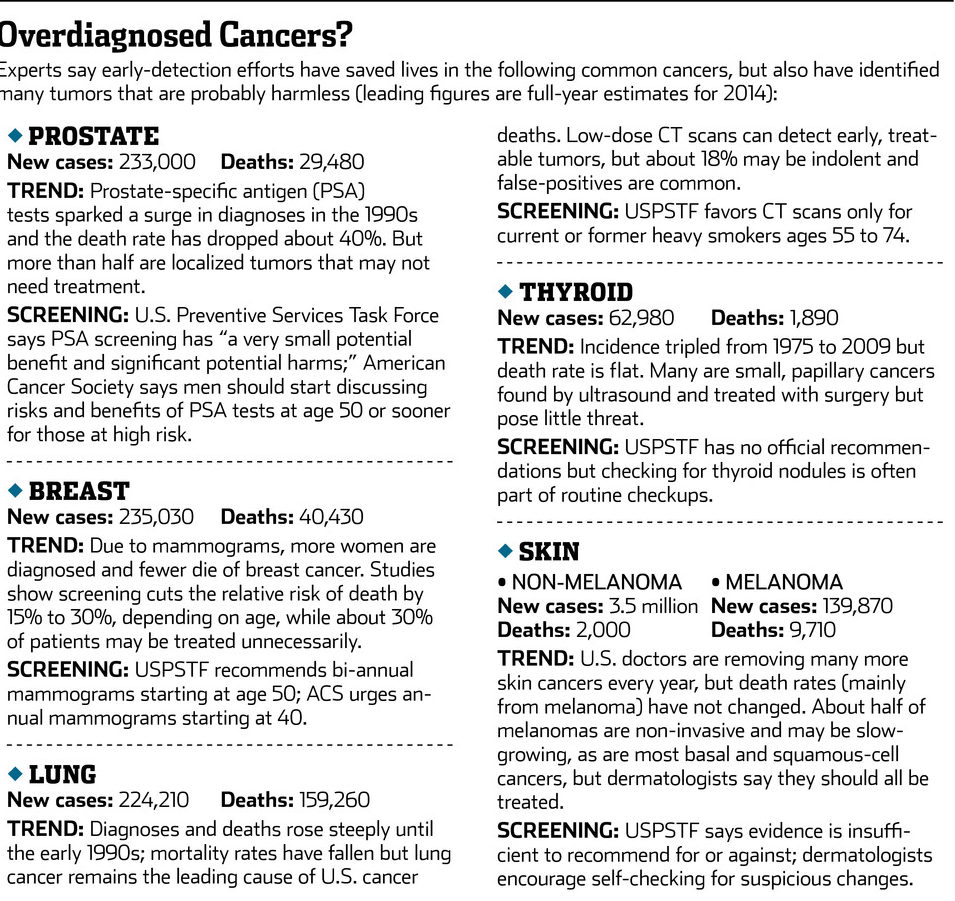
The idea that not all cancers are deadly is already beginning to transform treatment for prostate cancer. As many as 60% of the tumors detected via screening grow so slowly that they pose little threat in a man’s lifetime, experts say, and treating them with surgery or radiation carries a substantial risk of impotence or incontinence.
About 15% of patients now opt to monitor them instead—and some experts say more could probably do so safely.
Some urologists even propose calling prostate tumors with a Gleason score of 6 or below “benign lesions”—although others note that that would mean half of the men treated for prostate cancer in the past 20 years didn’t have cancer after all.
Overdiagnosis—the detection of tumors that aren’t likely to cause harm—is now a hot topic in other cancers as well. A growing volume of studies estimate that as many as 30% of invasive breast cancers, 18% of lung cancers and 90% of papillary thyroid cancers may not pose a lethal threat.
—Laura Esserman, A Breast-Cancer Surgeon At The University Of California, San Francisco
More than 2.5 million Americans are diagnosed with non-melanoma skin cancers each year—more than all other cancers combined. They are rarely fatal, and some experts say that removing the term “cancer” would encourage more doctors and patients to monitor the lesions rather than remove them surgically.
A commentary in the Journal of the American Medical Association last week noted that more than 100,000 people are treated for basal-cell cancers annually even though they died of other causes within a year. “Clinicians need to take a step back from the microscope and take a look at the patient,” the authors wrote.
Not So Fast
But such calls to rethink the C-word and slow the relentless drive for more and earlier treatments remain highly controversial.
Officials from five major dermatology societies have blasted the idea of calling non-melanoma skin cancers IDLEs, saying that deaths from squamous-cell cancers are rising and basal-cell carcinomas can invade surrounding tissues if untreated. “Renaming a destructive and sometimes fatal disease—to make it sound harmless—is a disservice to our patients,” the doctors wrote in Lancet Oncology.
Brett Coldiron, president of the American Academy of Dermatology, says it’s often the patients who want their skin cancers removed—”and sometimes you get surprised. These things that look like a basal-cell are a melanoma.”
Dr. Esserman and other doctors warning about overdiagnosis have been harshly debated at cancer meetings and have received angry letters from people convinced that early detection saved their lives, or could have saved loved ones.
Some critics say that the whole premise that cancers are over-diagnosed comes from statistical guesses, based on old, flawed studies, and that even if some patients are treated unnecessarily, early detection still saves lives.
“There’s no question that periodic screening doesn’t catch fast-growing cancers, but you save lives by finding moderate and slow-growing cancers and finding them earlier,” says Daniel Kopans, a senior radiologist at Massachusetts General Hospital.
Even doctors who accept the idea of overdiagnosis say it poses a dilemma when it comes to treating individual patients.
“I am confident that somewhere between 10% and 30% of women with localized invasive breast cancer would be just fine if we just watched them,” says Otis Brawley, chief medical officer of the American Cancer Society. “But I cannot look into a patient’s eyes and say, ‘You’re one of the 10% to 30% that should not be treated.’ “
The conflicting messages have left many patients bewildered. After years of educational campaigns saying that early detection saves lives, it’s no wonder that some people view recommendations to cut back on cancer screenings as dangerous, or veiled health-care rationing.
Bitter disputes still rage over a U.S. Preventive Services Task Force recommendation that men no longer use tests for prostate-specific antigen, or PSA, to screen for prostate cancer, and that women have mammograms every other year starting at age 50, rather than annually starting at 40, to reduce the likelihood of overdiagnosis.
At Congress’s insistence, the federal health law requires insurers to fully cover annual mammograms starting at 40 as part of “essential health benefits.”
“Everyone says they’d be willing to be overtreated if it means not dying—but that’s a big fallacy,” says Dr. Esserman. “By treating 1,000 people who have low-risk disease, we’re not going to save the one person with aggressive disease.”
Sharks And Goldfish
What makes scientists think some cancers are indolent? One clue comes from autopsies that find a substantial number of breast, thyroid, lung and other tumors that never caused symptoms in people who died of other causes.
Small, localized prostate cancers are so ubiquitous in older men that the risk is roughly equal to a man’s age: a 70-year-old has a 70% chance of harboring the disease. Yet the average lifetime risk of dying of prostate cancer is less than 3% according to the American Cancer Society.
Most of the evidence for overdiagnosis comes from statistical analyses of long-term cancer trends. Theoretically, as screening efforts find more early cancers, the death rate from those cancers should decline. Widespread use of colonoscopies and Pap smears has cut the death rate from colon and cervical cancers roughly in half since 1975.
But death rates from thyroid, kidney and skin cancers have stayed flat or increased, despite many more being diagnosed at early stages, leading researchers to conclude that many of those caught early would never have progressed.
Death rates from breast and prostate cancers have fallen by about 30% and about 40%, respectively, in the past 30 years. But experts disagree on whether that is due to the rise of screening mammograms and PSA tests or improved treatments.
“We have thrown the net very, very widely and eliminated some of the sharks,” says Ian Thompson, a urologist at University of Texas Health Science Center and co-chairman of the NCI advisory panel. “But we’ve also netted a lot of goldfish and assumed they’d behave the same way.”
The New War On Cancer
Part of the problem, says Dr. Brawley, is that modern medicine is using a definition of cancer that hasn’t changed since the 1850s, when German pathologists first described various types of the disease based on autopsy specimens.
Tiny lesions that would never have been detected a few decades ago are now routinely biopsied and analyzed, he says, “and if it looks just like what killed that woman 160 years ago, we assume it will be deadly today.”
But assuming cells that look the same will behave the same way is the biological equivalent of “racial profiling,” Dr. Brawley adds. Many other factors—including the tumor’s genetic profile and the patient’s immune system, diet and overall health—could affect how fast those cancer cells grow, or conceivably regress.
“We desperately need better tests to distinguish the things that will behave like traditional cancers versus the things that look like cancer but won’t,” Dr. Brawley says. “This is the beginning of the new war on cancer in the 21st century.”
Prodigious efforts are under way to devise such tests. The National Cancer Institute’s Early Detection Research Network is bringing together 300 investigators at 40 institutions to study how molecular patterns in screen-detected cancers differ from those that cause symptoms.
Biotech firms and university labs are also racing to develop prognostic tools.
Much progress has been made in identifying subtypes of tumors and tailoring treatments to them. “It’s a fallacy to throw up our hands and say we have no idea which patients are low risk,” says breast surgeon Shelley Hwang at Duke University Medical Center, who is also on the NCI panel.
Tests such as Genomic Health Inc.’s Oncotype DX and Agendia Inc.’s MammaPrint analyze patterns of gene activity on breast tumors that have been removed and can help predict how likely the cancer is to recur and whether the patient would benefit from chemotherapy after surgery.
Several new gene tests for prostate cancer have hit the market in the past year. Oncotype DX has a test that works at the biopsy stage and can help doctors assess how aggressive a particular tumor might be.
But clinicians say much more research needs to be done before they can say for certain how any individual cancer will behave. “I think we will get there. I just don’t think we’re there yet,” says Clifford Hudis, chief of breast-cancer medicine at Memorial Sloan Kettering Cancer Center in New York and past president of the American Society of Clinical Oncology.
Peace of Mind
In the absence of certainty, many doctors and patients are opting for more aggressive treatment, not less.
In breast cancer, for example, nearly 20% of women with early-stage tumors now elect to have both breasts removed, up from 3% in 1998“Patients do this for peace of mind, for symmetry—but there’s no survival benefit for most of them,” says Barbara Smith, director of the breast program at Massachusetts General Hospital.
About one-quarter of the breast cancers diagnosed each year aren’t technically cancers, but abnormal cells confined to milk ducts called “ductal carcinoma in situ” that were seldom noticed before mammography. Experts think only about 20% of DCIS lesions might eventually progress to become invasive cancer.
But they don’t know for sure, because virtually all DCIS cases are treated as if they are stage-one cancers, with lumpectomy or mastectomy, often combined with radiation.
“We are picking up on these conditions way before we know whether they are dangerous or not,” says Duke’s Dr. Hwang. “In our ignorance, it’s safest to assume they are all dangerous, but we’re hurting some women in the process.”
Few doctors dare leave DCIS untreated, but Dr. Hwang is leading a multicenter study treating patients who have small, estrogen-positive DCIS lesions with hormone therapy for six months in hopes they can avoid surgery.She hopes to start another study next year offering DCIS patients the option of hormone therapy or active surveillance alone. “We may identify a group of patients we could treat with just a pill rather than mastectomy,” she says.
Risk-Based Screening
Dr. Esserman is embarking on a major study to test a new approach to breast-cancer screening. She hopes to enroll 100,000 women from all five University of California medical centers and Sanford Health in North Dakota. Those with average risk will have mammograms every other year, starting at age 50.
Those at higher risk due to genetic variations, family history, dense breast tissue or other factors will be screened—with mammograms and other imaging tests—younger and more often.
“For some people, early detection does save lives—but we need to sort out who that might be,” says Dr. Esserman, who theorizes that after five years, such “risk-based screening” will have netted more high-risk cancers, fewer indolent ones and fewer false positives.
Any breast cancers that are diagnosed will be treated and tracked in registries shared among the universities; women with low-risk DCIS will be offered active surveillance, with or without hormone therapy, as well as surgical options.
The risks and benefits will be discussed in depth, and individual choices will be honored.
“For a woman with DCIS who has 6-year-old twins and a mother who died of breast cancer, the right option might be radical bilateral mastectomy,” says Dr. Esserman. “For someone who is 86 years old and has multiple co-morbidities, surveillance may be.”
Some critics, including Dr. Kopans, warn that risk-based screening could be risky, since about 75% of women diagnosed with breast cancers had no known risk factors.
Says Dr. Esserman: “We need to start testing some of these ideas, rather than just fighting over them. People are afraid to do less. We want to figure out how to do less safely.”
Related Articles:
Bitcoin Information & Resources (#GotBitcoin)
North Korea Infiltrates U.S. Remote Jobs—With The Help of Everyday Americans
America’s Leading Alien Hunters Depend On AI To Speed Their Search
Bitcoin’s Nouveau Riche Executives And Wealthy Investors In Search Of Ways To Protect Themselves
How Anthocyanins Shield Us From Microplastics
Origins Of Toxic Algae (Domoic Acid) Killing Sea Lions, Birds And Dolphins In Southern California
The Human Brain And It’s Ability To Time-Travel
Wall Street’s New Tariff Safe Haven: Biotech Companies Adopting Bitcoin Treasury Strategy
How Natural “Short Sleepers” Thrive On 4 Hours Of Sleep Per Night Thanks To A Gene Mutation
Nine Unknown Benefits of Sleep Including Penal And Clitoral Erections
Elite Athletes Try A New Training Tactic: More Vitamin D3
Bitcoin Industry On A Winning Streak As Sec. Drops Lawsuit After Lawsuit!!
FOIA Files: Elon Musk’s DOGE Wants A Heads Up On FOIA Requests
When Russia Came To Defend The United States
Ultimate Resource Covering DOGE AKA The Department of Government Efficiency
Your Money Is Currently Lawful. However, That Is Subject To Change #GotBitcoin #BitcoinFixesThis
Is The United Nations Going Bankrupt?
Bitcoin Industry Founders Should Stop Chasing Narratives And Start Creating Them
Consumer Finance Watchdog Finalizes ‘Open Banking’ Rules Aimed At Driving Competition
US Government Crypto Wallets Hacked For $20M — Arkham Intelligence
Coinbase Files FOIAs Against US Regulators Probing Banks’ Bitcoin Crackdown
The Botanist Daring To Ask: What If Plants Have Intelligence?
Theoretical Physicist Sylvester James Gates
FOIA Request Reveals SEC’s Gensler, Lawmakers Target Of Violent Threats
Ultimate Resource For Prediction Markets Covering Politics, Pop Culture, Sports And More
September (AKA Rektember) Is Once Again A Tough Month For Stocks AND Bitcoin
Ultimate Resource For Cloning humans. Biological, Ethical, And Social Considerations
FOIA Reveals Aurora Borealis Imperiled US Infrastructure From Power Grids To Satellites (5-10-2024)
Ultimate Resource Covering How “Silent Payments” Are Bringing New Privacy Protections To Bitcoin
Nostr Allows Bitcoiners To Build-Out A Decentralized, CENSORSHIP-RESISTANT Social-Media!!
Joe Rogan: I Have A Lot Of Hope For Bitcoin
Teen Cyber Prodigy Stumbled Onto Flaw Letting Him Hijack Teslas
Spyware Finally Got Scary Enough To Freak Lawmakers Out—After It Spied On Them
The First Nuclear-Powered Bitcoin Mine Is Here. Maybe It Can Clean Up Energy FUD
The World’s Best Bitcoin Policies: How They Do It In 37 Nations
Tonga To Copy El Salvador’s Bill Making Bitcoin Legal Tender, Says Former MP
Wordle Is The New “Lingo” Turning Fans Into Argumentative Strategy Nerds
Prospering In The Pandemic, Some Feel Financial Guilt And Gratitude
Is Art Therapy The Path To Mental Well-Being?
New York, California, New Jersey, And Alabama Move To Ban ‘Forever Chemicals’ In Firefighting Foam
The Mystery Of The Wasting House-Cats
What Pet Owners Should Know About Chronic Kidney Disease In Dogs And Cats
Pets Score Company Perks As The ‘New Dependents’
Why Is My Cat Rubbing His Face In Ants?
Natural Cure For Hyperthyroidism In Cats Including How To Switch Him/Her To A Raw Food Diet
Ultimate Resource For Cat Lovers
FDA Approves First-Ever Arthritis Pain Management Drug For Cats
Ultimate Resource On Duke of York’s Prince Andrew And His Sex Scandal
Walmart Filings Reveal Plans To Create Cryptocurrency, NFTs
Bitcoin’s Dominance of Crypto Payments Is Starting To Erode
T-Mobile Says Hackers Stole Data On About 37 Million Customers
Jack Dorsey Announces Bitcoin Legal Defense Fund
More Than 100 Millionaires Signed An Open Letter Asking To Be Taxed More Heavily
Federal Regulator Says Credit Unions Can Partner With Bitcoin Providers
What’s Behind The Fascination With Smash-And-Grab Shoplifting?
Train Robberies Are A Problem In Los Angeles, And No One Agrees On How To Stop Them
US Stocks Historically Deliver Strong Gains In Fed Hike Cycles (GotBitcoin)
Ian Alexander Jr., Only Child of Regina King, Dies At Age 26
Amazon Ends Its Charity Donation Program Amazonsmile After Other Cost-Cutting Efforts
BTC Panics, Then Jeers at DOJ Announcement of ‘Major Action’ Against Tiny Chinese Exchange Bitzlato
Indexing Is Coming To BTC Funds Via Decentralized Exchanges
Doctors Show Implicit Bias Towards Black Patients
Darkmail Pushes Privacy Into The Hands Of NSA-Weary Customers
3D Printing Make Anything From Candy Bars To Hand Guns
Stealing The Blood Of The Young May Make You More Youthful
Henrietta Lacks And Her Remarkable Cells Will Finally See Some Payback
AL_A Wins Approval For World’s First Magnetized Fusion Power Plant
Want To Be Rich? Bitcoin’s Limited Supply Cap Means You Only Need 0.01 BTC
Smart Money Is Buying Bitcoin Dip. Stocks, Not So Much
McDonald’s Jumps On Bitcoin Memewagon, Crypto Twitter Responds
America COMPETES Act Would Be Disastrous For Bitcoin Inustry (LOL) And More
Lyn Alden On Bitcoin, Inflation And The Potential Coming Energy Shock
Inflation And A Tale of Cantillionaires
El Salvador Plans Bill To Adopt Bitcoin As Legal Tender
Miami Mayor Says City Employees Should Be Able To Take Their Salaries In Bitcoin
Vast Troves of Classified Info Undermine National Security, Spy Chief Says
BREAKING: Arizona State Senator Introduces Bill To Make Bitcoin Legal Tender
San Francisco’s Historic Surveillance Law May Get Watered Down
How Bitcoin Contributions Funded A $1.4M Solar Installation In Zimbabwe
California Lawmaker Says National Privacy Law Is a Priority
The Pandemic Turbocharged Online Privacy Concerns
How To Protect Your Online Privacy While Working From Home
Researchers Use GPU Fingerprinting To Track Users Online
Japan’s $1 Trillion Bitcoin Industry May Ease Onerous Listing Rules
Ultimate Resource On A Weak / Strong Dollar’s Impact On Bitcoin
Fed Money Printer Goes Into Reverse (Quantitative Tightening): What Does It Mean For Crypto?
BTC Market Is Closer To A Bottom Than Stocks (#GotBitcoin)
When World’s Central Banks Get It Wrong, Guess Who Pays The Price??? (#GotBitcoin)
“Better Days Ahead With Crypto Deleveraging Coming To An End” — Joker
Bitcoin Funds Have Seen Record Investment Inflow In Recent Weeks
Bitcoin’s Epic Run Is Winning More Attention On Wall Street
Ultimate Resource For Bitcoin Industry Mergers And Acquisitions (M&A) (#GotBitcoin)
Why Wall Street Is Literally Salivating Over Bitcoin
Nasdaq-Listed MicroStrategy And Others Wary Of Looming Dollar Inflation, Turns To Bitcoin And Gold
Bitcoin For Corporations | Michael Saylor | Bitcoin Corporate Strategy
Ultimate Resource On Myanmar’s Involvement With Bitcoin Industry
‘I Cry Every Day’: Olympic Athletes Slam Food, COVID Tests And Conditions In Beijing
Does Your Baby’s Food Contain Toxic Metals? Here’s What Our Investigation Found
Ultimate Resource For Pro-Bitcoin Lobbying And Non-Profit Organizations
Ultimate Resource On BlockFi, Celsius And Nexo
Petition Calling For Resignation Of U.S. Securities/Exchange Commission Chair Gary Gensler
100 Million Americans Can Legally Bet on the Super Bowl. A Spot Bitcoin ETF? Forget About it!
Green Finance Isn’t Going Where It’s Needed
Shedding Some Light On The Murky World Of ESG Metrics
SEC Targets Greenwashers To Bring Law And Order To ESG
BlackRock (Assets Under Management $7.4 Trillion) CEO: Bitcoin Has Caught Our Attention
Canada’s Major Banks Go Offline In Mysterious (Bank Run?) Hours-Long Outage (#GotBitcoin)
On-Chain Data: A Framework To Evaluate Bitcoin
On Its 14th Birthday, Bitcoin’s 1,690,706,971% Gain Looks Kind of… Well Insane
The Most Important Health Metric Is Now At Your Fingertips
American Bargain Hunters Flock To A New Online Platform Forged In China
Why We Should Welcome Another Crypto Winter
Traders Prefer Gold, Fiat Safe Havens Over Bitcoin As Russia Goes To War
Music Distributor DistroKid Raises Money At $1.3 Billion Valuation
Nas Selling Rights To Two Songs Via Crypto Music Startup Royal
Ultimate Resource On Music Catalog Deals
Ultimate Resource On Music And NFTs And The Implications For The Entertainment Industry
Lead And Cadmium Could Be In Your Dark Chocolate
Catawba, Native-American Tribe Approves First Digital Economic Zone In The United States
The Miracle Of Blockchain’s Triple Entry Accounting
How And Why To Stimulate Your Vagus Nerve!
Housing Boom Brings A Shortage Of Land To Build New Homes
Biden Lays Out His Blueprint For Fair Housing
No Grave Dancing For Sam Zell Now. He’s Paying Up For Hot Properties
Cracks In The Housing Market Are Starting To Show
Ever-Growing Needs Strain U.S. Food Bank Operations
Food Pantry Helps Columbia Students Struggling To Pay Bills
Food Insecurity Driven By Climate Change Has Central Americans Fleeing To The U.S.
Housing Insecurity Is Now A Concern In Addition To Food Insecurity
Families Face Massive Food Insecurity Levels
US Troops Going Hungry (Food Insecurity) Is A National Disgrace
Everything You Should Know About Community Fridges, From Volunteering To Starting Your Own
Russia’s Independent Journalists Including Those Who Revealed The Pandora Papers Need Your Help
10 Women Who Used Crypto To Make A Difference In 2021
Happy International Women’s Day! Leaders Share Their Experiences In Crypto
Dollar On Course For Worst Performance In Over A Decade (#GotBitcoin)
Juice The Stock Market And Destroy The Dollar!! (#GotBitcoin)
Unusual Side Hustles You May Not Have Thought Of
Ultimate Resource On Global Inflation And Rising Interest Rates (#GotBitcoin)
The Fed Is Setting The Stage For Hyper-Inflation Of The Dollar (#GotBitcoin)
An Antidote To Inflation? ‘Buy Nothing’ Groups Gain Popularity
Why Is Bitcoin Dropping If It’s An ‘Inflation Hedge’?
Lyn Alden Talks Bitcoin, Inflation And The Potential Coming Energy Shock
Ultimate Resource On How Black Families Can Fight Against Rising Inflation (#GotBitcoin)
What The Fed’s Rate Hike Means For Inflation, Housing, Crypto And Stocks
Egyptians Buy Bitcoin Despite Prohibitive New Banking Laws
Archaeologists Uncover Five Tombs In Egypt’s Saqqara Necropolis
History of Alchemy From Ancient Egypt To Modern Times
Former World Bank Chief Didn’t Act On Warnings Of Sexual Harassment
Does Your Hospital or Doctor Have A Financial Relationship With Big Pharma?
Ultimate Resource Covering The Crisis Taking Place In The Nickel Market
Apple Along With Meta And Secret Service Agents Fooled By Law Enforcement Impersonators
Handy Tech That Can Support Your Fitness Goals
How To Naturally Increase Your White Blood Cell Count
Ultimate Source For Russians Oligarchs And The Impact Of Sanctions On Them
Ultimate Source For Bitcoin Price Manipulation By Wall Street
Russia, Sri Lanka And Lebanon’s Defaults Could Be The First Of Many (#GotBitcoin)
Will Community Group Buying Work In The US?
Building And Running Businesses In The ‘Spirit Of Bitcoin’
What Is The Mysterious Liver Disease Hurting (And Killing) Children?
Citigroup Trader Is Scapegoat For Flash Crash In European Stocks (#GotBitcoin)
Bird Flu Outbreak Approaches Worst Ever In U.S. With 37 Million Animals Dead
Financial Inequality Grouped By Race For Blacks, Whites And Hispanics
How Black Businesses Can Prosper From Targeting A Trillion-Dollar Black Culture Market (#GotBitcoin)
Ultimate Resource For Central Bank Digital Currencies (#GotBitcoin) Page#2
Meet The Crypto Angel Investor Running For Congress In Nevada (#GotBitcoin?)
Introducing BTCPay Vault – Use Any Hardware Wallet With BTCPay And Its Full Node (#GotBitcoin?)
How Not To Lose Your Coins In 2020: Alternative Recovery Methods (#GotBitcoin?)
H.R.5635 – Virtual Currency Tax Fairness Act of 2020 ($200.00 Limit) 116th Congress (2019-2020)
Adam Back On Satoshi Emails, Privacy Concerns And Bitcoin’s Early Days
The Prospect of Using Bitcoin To Build A New International Monetary System Is Getting Real
How To Raise Funds For Australia Wildfire Relief Efforts (Using Bitcoin And/Or Fiat )
Former Regulator Known As ‘Crypto Dad’ To Launch Digital-Dollar Think Tank (#GotBitcoin?)
Currency ‘Cold War’ Takes Center Stage At Pre-Davos Crypto Confab (#GotBitcoin?)
A Blockchain-Secured Home Security Camera Won Innovation Awards At CES 2020 Las Vegas
Bitcoin’s Had A Sensational 11 Years (#GotBitcoin?)
Sergey Nazarov And The Creation Of A Decentralized Network Of Oracles
Google Suspends MetaMask From Its Play App Store, Citing “Deceptive Services”
Christmas Shopping: Where To Buy With Crypto This Festive Season
At 8,990,000% Gains, Bitcoin Dwarfs All Other Investments This Decade
Coinbase CEO Armstrong Wins Patent For Tech Allowing Users To Email Bitcoin
Bitcoin Has Got Society To Think About The Nature Of Money
How DeFi Goes Mainstream In 2020: Focus On Usability (#GotBitcoin?)
Dissidents And Activists Have A Lot To Gain From Bitcoin, If Only They Knew It (#GotBitcoin?)
At A Refugee Camp In Iraq, A 16-Year-Old Syrian Is Teaching Crypto Basics
Bitclub Scheme Busted In The US, Promising High Returns From Mining
Bitcoin Advertised On French National TV
Germany: New Proposed Law Would Legalize Banks Holding Bitcoin
How To Earn And Spend Bitcoin On Black Friday 2019
The Ultimate List of Bitcoin Developments And Accomplishments
Charities Put A Bitcoin Twist On Giving Tuesday
Family Offices Finally Accept The Benefits of Investing In Bitcoin
An Army Of Bitcoin Devs Is Battle-Testing Upgrades To Privacy And Scaling
Bitcoin ‘Carry Trade’ Can Net Annual Gains With Little Risk, Says PlanB
Max Keiser: Bitcoin’s ‘Self-Settlement’ Is A Revolution Against Dollar
Blockchain Can And Will Replace The IRS
China Seizes The Blockchain Opportunity. How Should The US Respond? (#GotBitcoin?)
Jack Dorsey: You Can Buy A Fraction Of Berkshire Stock Or ‘Stack Sats’
Bitcoin Price Skyrockets $500 In Minutes As Bakkt BTC Contracts Hit Highs
Bitcoin’s Irreversibility Challenges International Private Law: Legal Scholar
Bitcoin Has Already Reached 40% Of Average Fiat Currency Lifespan
Yes, Even Bitcoin HODLers Can Lose Money In The Long-Term: Here’s How (#GotBitcoin?)
Unicef To Accept Donations In Bitcoin (#GotBitcoin?)
Former Prosecutor Asked To “Shut Down Bitcoin” And Is Now Face Of Crypto VC Investing (#GotBitcoin?)
Switzerland’s ‘Crypto Valley’ Is Bringing Blockchain To Zurich
Next Bitcoin Halving May Not Lead To Bull Market, Says Bitmain CEO
Bitcoin Developer Amir Taaki, “We Can Crash National Economies” (#GotBitcoin?)
Veteran Crypto And Stocks Trader Shares 6 Ways To Invest And Get Rich
Is Chainlink Blazing A Trail Independent Of Bitcoin?
Nearly $10 Billion In BTC Is Held In Wallets Of 8 Crypto Exchanges (#GotBitcoin?)
SEC Enters Settlement Talks With Alleged Fraudulent Firm Veritaseum (#GotBitcoin?)
Blockstream’s Samson Mow: Bitcoin’s Block Size Already ‘Too Big’
Attorneys Seek Bank Of Ireland Execs’ Testimony Against OneCoin Scammer (#GotBitcoin?)
OpenLibra Plans To Launch Permissionless Fork Of Facebook’s Stablecoin (#GotBitcoin?)
Tiny $217 Options Trade On Bitcoin Blockchain Could Be Wall Street’s Death Knell (#GotBitcoin?)
Class Action Accuses Tether And Bitfinex Of Market Manipulation (#GotBitcoin?)
Sharia Goldbugs: How ISIS Created A Currency For World Domination (#GotBitcoin?)
Bitcoin Eyes Demand As Hong Kong Protestors Announce Bank Run (#GotBitcoin?)
How To Securely Transfer Crypto To Your Heirs
‘Gold-Backed’ Crypto Token Promoter Karatbars Investigated By Florida Regulators (#GotBitcoin?)
Crypto News From The Spanish-Speaking World (#GotBitcoin?)
Financial Services Giant Morningstar To Offer Ratings For Crypto Assets (#GotBitcoin?)
‘Gold-Backed’ Crypto Token Promoter Karatbars Investigated By Florida Regulators (#GotBitcoin?)
The Original Sins Of Cryptocurrencies (#GotBitcoin?)
Bitcoin Is The Fraud? JPMorgan Metals Desk Fixed Gold Prices For Years (#GotBitcoin?)
Israeli Startup That Allows Offline Crypto Transactions Secures $4M (#GotBitcoin?)
[PSA] Non-genuine Trezor One Devices Spotted (#GotBitcoin?)
Bitcoin Stronger Than Ever But No One Seems To Care: Google Trends (#GotBitcoin?)
First-Ever SEC-Qualified Token Offering In US Raises $23 Million (#GotBitcoin?)
You Can Now Prove A Whole Blockchain With One Math Problem – Really
Crypto Mining Supply Fails To Meet Market Demand In Q2: TokenInsight
$2 Billion Lost In Mt. Gox Bitcoin Hack Can Be Recovered, Lawyer Claims (#GotBitcoin?)
Fed Chair Says Agency Monitoring Crypto But Not Developing Its Own (#GotBitcoin?)
Wesley Snipes Is Launching A Tokenized $25 Million Movie Fund (#GotBitcoin?)
Mystery 94K BTC Transaction Becomes Richest Non-Exchange Address (#GotBitcoin?)
A Crypto Fix For A Broken International Monetary System (#GotBitcoin?)
Four Out Of Five Top Bitcoin QR Code Generators Are Scams: Report (#GotBitcoin?)
Waves Platform And The Abyss To Jointly Launch Blockchain-Based Games Marketplace (#GotBitcoin?)
Bitmain Ramps Up Power And Efficiency With New Bitcoin Mining Machine (#GotBitcoin?)
Ledger Live Now Supports Over 1,250 Ethereum-Based ERC-20 Tokens (#GotBitcoin?)
Miss Finland: Bitcoin’s Risk Keeps Most Women Away From Cryptocurrency (#GotBitcoin?)
Artist Akon Loves BTC And Says, “It’s Controlled By The People” (#GotBitcoin?)
Ledger Live Now Supports Over 1,250 Ethereum-Based ERC-20 Tokens (#GotBitcoin?)
Co-Founder Of LinkedIn Presents Crypto Rap Video: Hamilton Vs. Satoshi (#GotBitcoin?)
Crypto Insurance Market To Grow, Lloyd’s Of London And Aon To Lead (#GotBitcoin?)
No ‘AltSeason’ Until Bitcoin Breaks $20K, Says Hedge Fund Manager (#GotBitcoin?)
NSA Working To Develop Quantum-Resistant Cryptocurrency: Report (#GotBitcoin?)
Custody Provider Legacy Trust Launches Crypto Pension Plan (#GotBitcoin?)
Vaneck, SolidX To Offer Limited Bitcoin ETF For Institutions Via Exemption (#GotBitcoin?)
Russell Okung: From NFL Superstar To Bitcoin Educator In 2 Years (#GotBitcoin?)
Bitcoin Miners Made $14 Billion To Date Securing The Network (#GotBitcoin?)
Why Does Amazon Want To Hire Blockchain Experts For Its Ads Division?
Argentina’s Economy Is In A Technical Default (#GotBitcoin?)
Blockchain-Based Fractional Ownership Used To Sell High-End Art (#GotBitcoin?)
Portugal Tax Authority: Bitcoin Trading And Payments Are Tax-Free (#GotBitcoin?)
Bitcoin ‘Failed Safe Haven Test’ After 7% Drop, Peter Schiff Gloats (#GotBitcoin?)
Bitcoin Dev Reveals Multisig UI Teaser For Hardware Wallets, Full Nodes (#GotBitcoin?)
Bitcoin Price: $10K Holds For Now As 50% Of CME Futures Set To Expire (#GotBitcoin?)
Bitcoin Realized Market Cap Hits $100 Billion For The First Time (#GotBitcoin?)
Stablecoins Begin To Look Beyond The Dollar (#GotBitcoin?)
Bank Of England Governor: Libra-Like Currency Could Replace US Dollar (#GotBitcoin?)
Binance Reveals ‘Venus’ — Its Own Project To Rival Facebook’s Libra (#GotBitcoin?)
The Real Benefits Of Blockchain Are Here. They’re Being Ignored (#GotBitcoin?)
CommBank Develops Blockchain Market To Boost Biodiversity (#GotBitcoin?)
SEC Approves Blockchain Tech Startup Securitize To Record Stock Transfers (#GotBitcoin?)
SegWit Creator Introduces New Language For Bitcoin Smart Contracts (#GotBitcoin?)
You Can Now Earn Bitcoin Rewards For Postmates Purchases (#GotBitcoin?)
Bitcoin Price ‘Will Struggle’ In Big Financial Crisis, Says Investor (#GotBitcoin?)
Fidelity Charitable Received Over $100M In Crypto Donations Since 2015 (#GotBitcoin?)
Would Blockchain Better Protect User Data Than FaceApp? Experts Answer (#GotBitcoin?)
Just The Existence Of Bitcoin Impacts Monetary Policy (#GotBitcoin?)
What Are The Biggest Alleged Crypto Heists And How Much Was Stolen? (#GotBitcoin?)
IRS To Cryptocurrency Owners: Come Clean, Or Else!
Coinbase Accidentally Saves Unencrypted Passwords Of 3,420 Customers (#GotBitcoin?)
Bitcoin Is A ‘Chaos Hedge, Or Schmuck Insurance‘ (#GotBitcoin?)
Bakkt Announces September 23 Launch Of Futures And Custody
Coinbase CEO: Institutions Depositing $200-400M Into Crypto Per Week (#GotBitcoin?)
Researchers Find Monero Mining Malware That Hides From Task Manager (#GotBitcoin?)
Crypto Dusting Attack Affects Nearly 300,000 Addresses (#GotBitcoin?)
A Case For Bitcoin As Recession Hedge In A Diversified Investment Portfolio (#GotBitcoin?)
SEC Guidance Gives Ammo To Lawsuit Claiming XRP Is Unregistered Security (#GotBitcoin?)
15 Countries To Develop Crypto Transaction Tracking System: Report (#GotBitcoin?)
US Department Of Commerce Offering 6-Figure Salary To Crypto Expert (#GotBitcoin?)
Mastercard Is Building A Team To Develop Crypto, Wallet Projects (#GotBitcoin?)
Canadian Bitcoin Educator Scams The Scammer And Donates Proceeds (#GotBitcoin?)
Amazon Wants To Build A Blockchain For Ads, New Job Listing Shows (#GotBitcoin?)
Shield Bitcoin Wallets From Theft Via Time Delay (#GotBitcoin?)
Blockstream Launches Bitcoin Mining Farm With Fidelity As Early Customer (#GotBitcoin?)
Commerzbank Tests Blockchain Machine To Machine Payments With Daimler (#GotBitcoin?)
Man Takes Bitcoin Miner Seller To Tribunal Over Electricity Bill And Wins (#GotBitcoin?)
Bitcoin’s Computing Power Sets Record As Over 100K New Miners Go Online (#GotBitcoin?)
Walmart Coin And Libra Perform Major Public Relations For Bitcoin (#GotBitcoin?)
Judge Says Buying Bitcoin Via Credit Card Not Necessarily A Cash Advance (#GotBitcoin?)
Poll: If You’re A Stockowner Or Crypto-Currency Holder. What Will You Do When The Recession Comes?
1 In 5 Crypto Holders Are Women, New Report Reveals (#GotBitcoin?)
Beating Bakkt, Ledgerx Is First To Launch ‘Physical’ Bitcoin Futures In Us (#GotBitcoin?)
Facebook Warns Investors That Libra Stablecoin May Never Launch (#GotBitcoin?)
Government Money Printing Is ‘Rocket Fuel’ For Bitcoin (#GotBitcoin?)
Bitcoin-Friendly Square Cash App Stock Price Up 56% In 2019 (#GotBitcoin?)
Safeway Shoppers Can Now Get Bitcoin Back As Change At 894 US Stores (#GotBitcoin?)
TD Ameritrade CEO: There’s ‘Heightened Interest Again’ With Bitcoin (#GotBitcoin?)
Venezuela Sets New Bitcoin Volume Record Thanks To 10,000,000% Inflation (#GotBitcoin?)
Newegg Adds Bitcoin Payment Option To 73 More Countries (#GotBitcoin?)
China’s Schizophrenic Relationship With Bitcoin (#GotBitcoin?)
More Companies Build Products Around Crypto Hardware Wallets (#GotBitcoin?)
Bakkt Is Scheduled To Start Testing Its Bitcoin Futures Contracts Today (#GotBitcoin?)
Bitcoin Network Now 8 Times More Powerful Than It Was At $20K Price (#GotBitcoin?)
Crypto Exchange BitMEX Under Investigation By CFTC: Bloomberg (#GotBitcoin?)
“Bitcoin An ‘Unstoppable Force,” Says US Congressman At Crypto Hearing (#GotBitcoin?)
Bitcoin Network Is Moving $3 Billion Daily, Up 210% Since April (#GotBitcoin?)
Cryptocurrency Startups Get Partial Green Light From Washington
Fundstrat’s Tom Lee: Bitcoin Pullback Is Healthy, Fewer Searches Аre Good (#GotBitcoin?)
Bitcoin Lightning Nodes Are Snatching Funds From Bad Actors (#GotBitcoin?)
The Provident Bank Now Offers Deposit Services For Crypto-Related Entities (#GotBitcoin?)
Bitcoin Could Help Stop News Censorship From Space (#GotBitcoin?)
US Sanctions On Iran Crypto Mining — Inevitable Or Impossible? (#GotBitcoin?)
US Lawmaker Reintroduces ‘Safe Harbor’ Crypto Tax Bill In Congress (#GotBitcoin?)
EU Central Bank Won’t Add Bitcoin To Reserves — Says It’s Not A Currency (#GotBitcoin?)
The Miami Dolphins Now Accept Bitcoin And Litecoin Crypt-Currency Payments (#GotBitcoin?)
Trump Bashes Bitcoin And Alt-Right Is Mad As Hell (#GotBitcoin?)
Goldman Sachs Ramps Up Development Of New Secret Crypto Project (#GotBitcoin?)
Blockchain And AI Bond, Explained (#GotBitcoin?)
Grayscale Bitcoin Trust Outperformed Indexes In First Half Of 2019 (#GotBitcoin?)
XRP Is The Worst Performing Major Crypto Of 2019 (GotBitcoin?)
Bitcoin Back Near $12K As BTC Shorters Lose $44 Million In One Morning (#GotBitcoin?)
As Deutsche Bank Axes 18K Jobs, Bitcoin Offers A ‘Plan ฿”: VanEck Exec (#GotBitcoin?)
Argentina Drives Global LocalBitcoins Volume To Highest Since November (#GotBitcoin?)
‘I Would Buy’ Bitcoin If Growth Continues — Investment Legend Mobius (#GotBitcoin?)
Lawmakers Push For New Bitcoin Rules (#GotBitcoin?)
Facebook’s Libra Is Bad For African Americans (#GotBitcoin?)
Crypto Firm Charity Announces Alliance To Support Feminine Health (#GotBitcoin?)
Canadian Startup Wants To Upgrade Millions Of ATMs To Sell Bitcoin (#GotBitcoin?)
Trump Says US ‘Should Match’ China’s Money Printing Game (#GotBitcoin?)
Casa Launches Lightning Node Mobile App For Bitcoin Newbies (#GotBitcoin?)
Bitcoin Rally Fuels Market In Crypto Derivatives (#GotBitcoin?)
World’s First Zero-Fiat ‘Bitcoin Bond’ Now Available On Bloomberg Terminal (#GotBitcoin?)
Buying Bitcoin Has Been Profitable 98.2% Of The Days Since Creation (#GotBitcoin?)
Another Crypto Exchange Receives License For Crypto Futures
From ‘Ponzi’ To ‘We’re Working On It’ — BIS Chief Reverses Stance On Crypto (#GotBitcoin?)
These Are The Cities Googling ‘Bitcoin’ As Interest Hits 17-Month High (#GotBitcoin?)
Venezuelan Explains How Bitcoin Saves His Family (#GotBitcoin?)
Quantum Computing Vs. Blockchain: Impact On Cryptography
This Fund Is Riding Bitcoin To Top (#GotBitcoin?)
Bitcoin’s Surge Leaves Smaller Digital Currencies In The Dust (#GotBitcoin?)
Bitcoin Exchange Hits $1 Trillion In Trading Volume (#GotBitcoin?)
Bitcoin Breaks $200 Billion Market Cap For The First Time In 17 Months (#GotBitcoin?)
You Can Now Make State Tax Payments In Bitcoin (#GotBitcoin?)
Religious Organizations Make Ideal Places To Mine Bitcoin (#GotBitcoin?)
Goldman Sacs And JP Morgan Chase Finally Concede To Crypto-Currencies (#GotBitcoin?)
Bitcoin Heading For Fifth Month Of Gains Despite Price Correction (#GotBitcoin?)
Breez Reveals Lightning-Powered Bitcoin Payments App For IPhone (#GotBitcoin?)
Big Four Auditing Firm PwC Releases Cryptocurrency Auditing Software (#GotBitcoin?)
Amazon-Owned Twitch Quietly Brings Back Bitcoin Payments (#GotBitcoin?)
JPMorgan Will Pilot ‘JPM Coin’ Stablecoin By End Of 2019: Report (#GotBitcoin?)
Is There A Big Short In Bitcoin? (#GotBitcoin?)
Coinbase Hit With Outage As Bitcoin Price Drops $1.8K In 15 Minutes
Samourai Wallet Releases Privacy-Enhancing CoinJoin Feature (#GotBitcoin?)
There Are Now More Than 5,000 Bitcoin ATMs Around The World (#GotBitcoin?)
You Can Now Get Bitcoin Rewards When Booking At Hotels.Com (#GotBitcoin?)
North America’s Largest Solar Bitcoin Mining Farm Coming To California (#GotBitcoin?)
Bitcoin On Track For Best Second Quarter Price Gain On Record (#GotBitcoin?)
Bitcoin Hash Rate Climbs To New Record High Boosting Network Security (#GotBitcoin?)
Bitcoin Exceeds 1Million Active Addresses While Coinbase Custodies $1.3B In Assets
Why Bitcoin’s Price Suddenly Surged Back $5K (#GotBitcoin?)
Zebpay Becomes First Exchange To Add Lightning Payments For All Users (#GotBitcoin?)
Coinbase’s New Customer Incentive: Interest Payments, With A Crypto Twist (#GotBitcoin?)
The Best Bitcoin Debit (Cashback) Cards Of 2019 (#GotBitcoin?)
Real Estate Brokerages Now Accepting Bitcoin (#GotBitcoin?)
Ernst & Young Introduces Tax Tool For Reporting Cryptocurrencies (#GotBitcoin?)
Recession Is Looming, or Not. Here’s How To Know (#GotBitcoin?)
How Will Bitcoin Behave During A Recession? (#GotBitcoin?)
Many U.S. Financial Officers Think a Recession Will Hit Next Year (#GotBitcoin?)
Definite Signs of An Imminent Recession (#GotBitcoin?)
What A Recession Could Mean for Women’s Unemployment (#GotBitcoin?)
Investors Run Out of Options As Bitcoin, Stocks, Bonds, Oil Cave To Recession Fears (#GotBitcoin?)
Goldman Is Looking To Reduce “Marcus” Lending Goal On Credit (Recession) Caution (#GotBitcoin?)
Your Questions And Comments Are Greatly Appreciated.
Monty H. & Carolyn A.
Go back
Leave a Reply
You must be logged in to post a comment.